Atypical femoral fracture
Definition
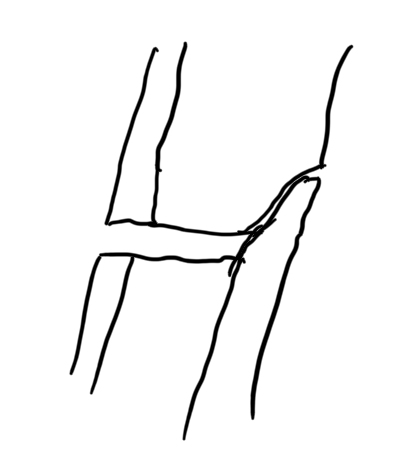
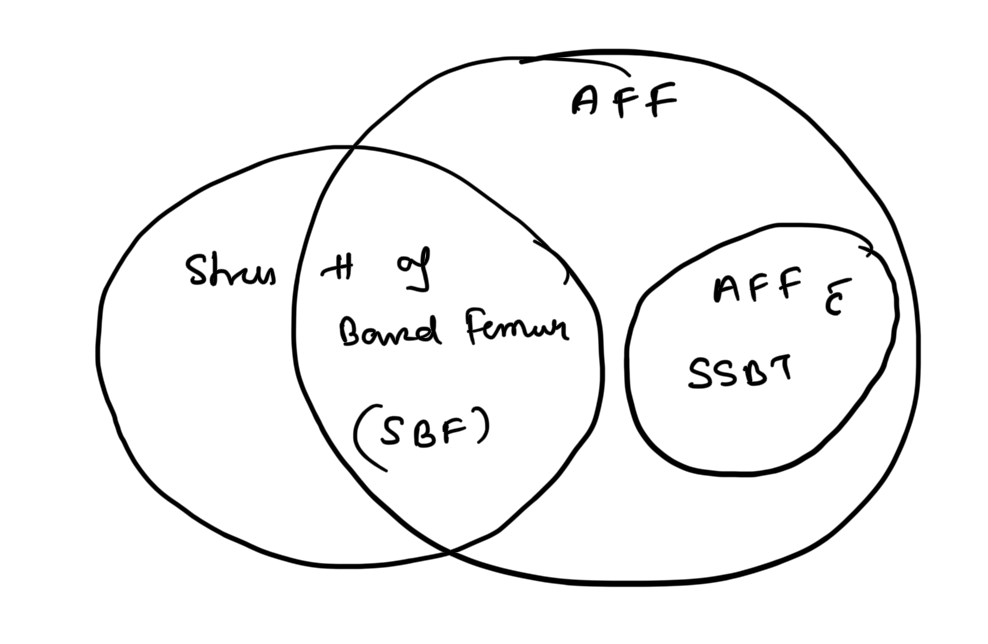
Atypical femoral fractures are rare stress fractures that occur in the subtrochanteric or diaphyseal region of the femur, most often on the lateral cortex.
They are associated with minimal or no trauma and often linked to long-term bisphosphonate use or other bone metabolism disorders.
Source: American Society for Bone and Mineral Research (ASBMR) Criteria
ASBMR Diagnostic Criteria (Major & Minor)
To diagnose AFF, 4 out of 5 major features should be present.
Major Features
- Minimal or no trauma (e.g., fall from standing height or less)
- Fracture originates at the lateral cortex; may be transverse or short oblique
- Complete fracture involves both cortices, may have medial spike
- Incomplete fracture involves only the lateral cortex
- Incomplete fracture involves only the lateral cortex
- Non- or minimally comminuted fracture
- Localized periosteal or endosteal thickening (“beaking” or “flaring”) of the lateral cortex
Minor Features
(Not required for diagnosis but often associated)
- Bilateral fractures and symptoms
- Delayed healing
- Comorbidities or medication use
History & Risk Factors
- Comorbidities
- Collagen diseases (e.g., Rheumatoid arthritis)
- Chronic obstructive pulmonary disease (COPD)
- Nutritional Deficiency
- Low calcium or Vitamin D levels
- Medications
- Bisphosphonates (long-term use)
- PPIs
- Glucocorticoids
Investigations
- X-ray:
- Shows focal cortical thickening at the lateral cortex
- Transverse fracture pattern
- MRI / Bone Scan:
- Detects stress reaction or incomplete fractures
- DEXA Scan:
- Evaluate bone mineral density
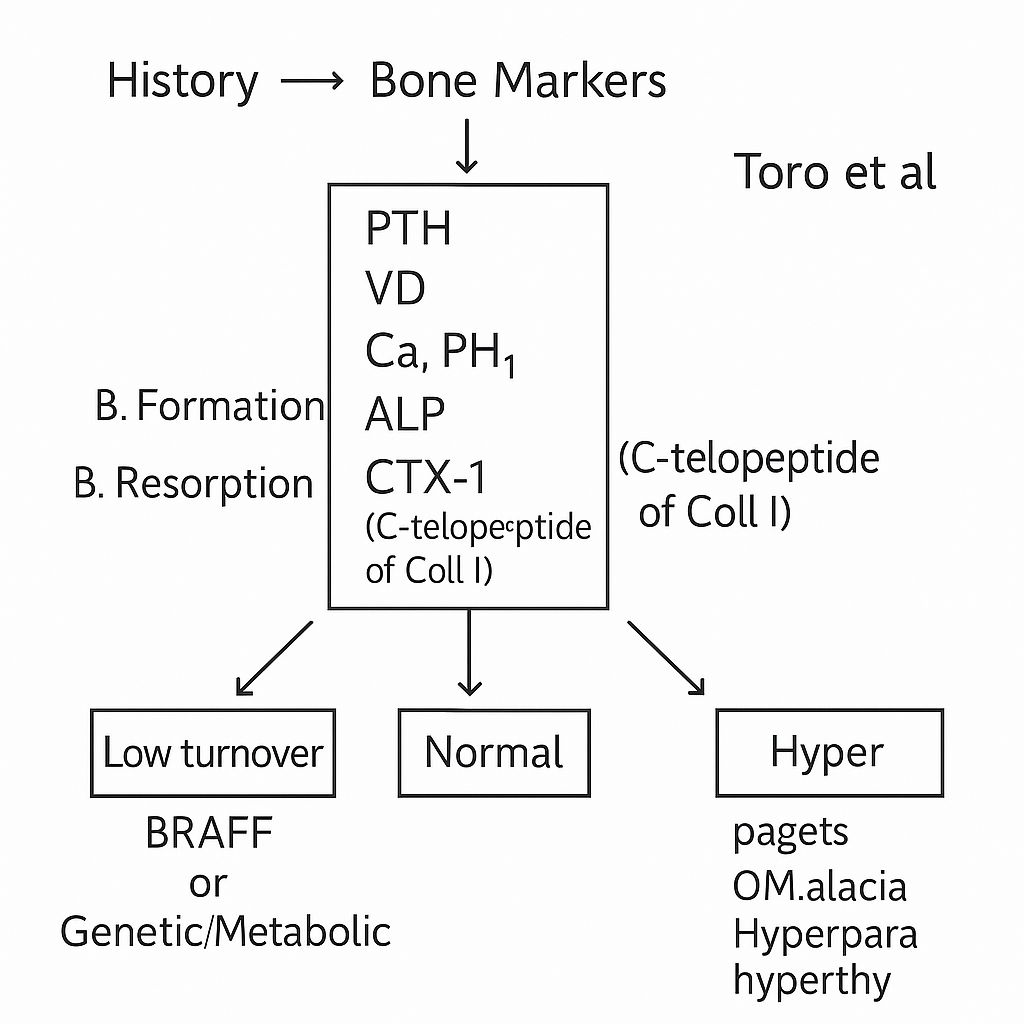
- Biochemical Work-up:
- Serum calcium, phosphate, Vitamin D, PTH, and bone turnover markers
Pathophysiology
- Reduced bone turnover (due to bisphosphonate suppression of osteoclast activity)
- Low bone geometry adaptation (increased tensile stress at lateral cortex)
- Other contributing factors:
- Mechanical stress
- Drugs
- Comorbidities
Clinical Features
| Type | Pain | Fracture Type | Progression |
|---|---|---|---|
| Complete | Pain present | Transverse | Non-comminuted |
| Incomplete | Pain may be present | Lateral cortex only | May progress to complete fracture |
Symptoms
- Dull aching pain in thigh or groin
- Often bilateral
- May precede fracture by weeks to months
Management
Non-Operative (Incomplete Fracture without pain)
- Discontinue bisphosphonate therapy
- Start Calcium and Vitamin D supplementation
- Teriparatide (Parathyroid hormone analog) for bone remodeling
- Protected weight-bearing or rest
Operative Management
- Intramedullary (IM) nailing: preferred for complete or painful incomplete fractures
- Provides full-length protection of femur
- Complications:
- Hardware failure
- Delayed or non-union
- Plating: reserved for cases with very narrow femoral canal or poor bone stock
Approach
Clinical Scenarios
| Finding | Pain | Management |
|---|---|---|
| No fracture (stress reaction) | Present | Rest, vitamin D, stop bisphosphonate |
| Incomplete fracture | Painful | Prophylactic IM nailing |
| Complete fracture | Painful | IM nail fixation |
Oh et al. (Japan):
Summary Points
- AFF = Atypical, low-energy, lateral cortical stress fracture
- Common in long-term bisphosphonate users
- ASBMR: 4 of 5 major criteria required for diagnosis
- Management: Stop bisphosphonate, supplement Ca + Vit D, consider IM nail